UT study finds decline in reproductive healthcare quality post-Roe v. Wade
June 8, 2023
The quality of care provided to patients experiencing pregnancy complications, often treated by abortion, has decreased since the reversal of Roe v. Wade, according to a study published on May 15 by researchers from UT’s Texas Policy Evaluation Project.
Since the U.S. Supreme Court overturned Roe v. Wade last June, it has become harder for doctors to provide their patients with the typical standard of care, TxPEP spokesperson Laura Dixon said in an email. The typical standard of care for the cases presented in the study is abortion. According to Dixon, restrictive laws lead to “worsened health outcomes” because legislation limits medical providers’ judgment.
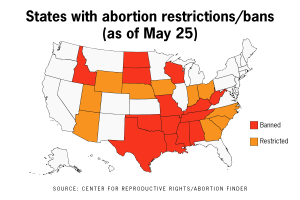
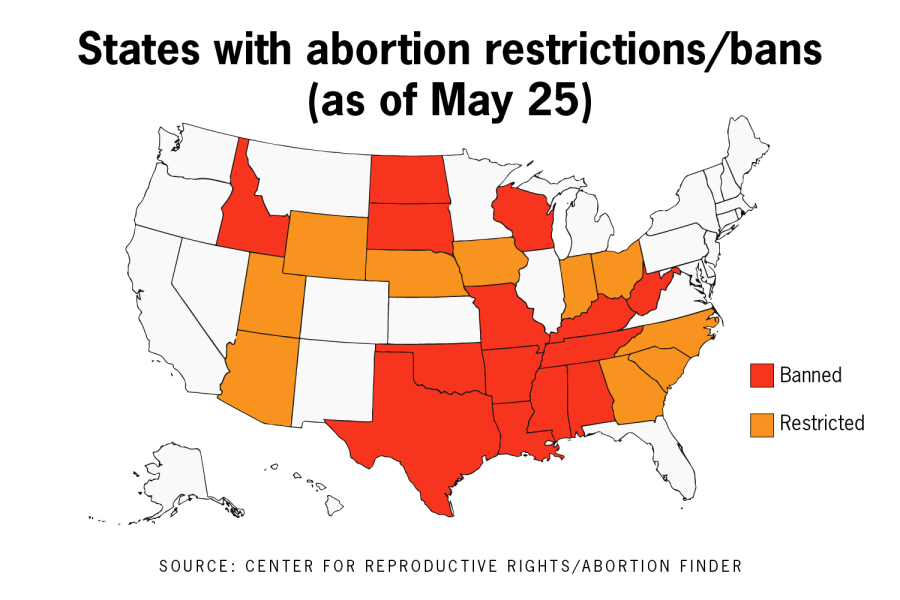
The study, named “Care Post-Roe,” analyzed 50 submissions from healthcare providers in states with restrictive abortion laws, removing some information to avoid identifying participants. The study submissions show the new legal uncertainties healthcare teams must navigate when caring for pregnant patients. In one case, an anesthesiologist refused to give an epidural to a patient experiencing birthing complications.
“They believed that providing an epidural could be considered [a crime] under the new law,” the submission said. “The patient received some IV morphine instead and delivered a few hours later but was very uncomfortable through the remainder of her labor.”
Other narratives presented in the study provide details of travel, accommodation and medical expenses when patients left restrictive states to obtain necessary care. The high costs, paired with an unfamiliar operating doctor, convinced some patients from the study to carry their pregnancy to term despite fetal anomalies.
“[The] patient said to me, ‘It is really easy for doctors to suggest (abortion), but they don’t realize how hard it is,’” one submission said. “It is frustrating that the patient had to consider so many non-medical issues when deciding which plan of care she wanted.”
Dixon said patients should be able to trust their doctor’s medical judgment when making reproductive health decisions. However, she said abortion laws prohibiting doctors “to offer evidence-based pregnancy care” have the greatest impact in states with poor maternal health, like Texas.
“It’s not about clarifying into law the exceptions,” Dixon said. “It’s about letting providers use their clinical expertise and patients indicating their preference for care based on that information that should be guiding medical decisions.”
Five women filed a lawsuit in March against the State of Texas to seek clarity on the state’s “medical emergency” exemption. Each woman was denied an abortion despite “dangerous pregnancy complications,” according to a press release from the Center for Reproductive Rights. The number of plaintiffs in that case has grown to 15 and now includes healthcare providers and patients.
According to an email from Sarah Wheat, a spokesperson for Planned Parenthood of Greater Texas, some medical conditions can quickly become life-threatening for pregnant women.
“Texans need access to medication and surgical abortion and yet abortions are banned in Texas,” Wheat said. “This creates enormous challenges for Texans who can’t travel to another state to access an abortion.”
Wheat said Planned Parenthood expanded access to birth control services at select Texas health centers and continues to provide STI testing and treatment, among other preventative screenings.
“Texas’ statewide abortion ban puts pregnant women’s health at risk,” Wheat said. “We’d like to see expanded access to healthcare for Texans instead of the barriers to care that many Texans face.”